In the USA, Black women have the highest mortality from breast cancer of any other group, despite the rate of diagnosis of breast cancer being highest in White women. Hispanic women have a lower breast cancer diagnosis incidence than either, but mortality rates are disproportionately high in Hispanic women also. Here are the CDC incidence and mortality statistics over time:
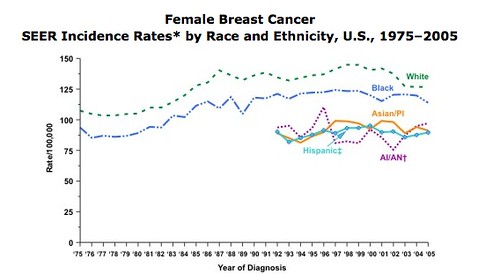
“Incidence rate” means how many women out of a given number get the disease each year. The graph below shows how many women out of 100,000 got breast cancer each year during the years 1975–2005. The year 2005 is the most recent year for which numbers have been reported. The breast cancer incidence rate is grouped by race and ethnicity.
For example, you can see that white women had the highest incidence rate for breast cancer. Black women had the second highest incidence of getting breast cancer, followed by American Indian/Alaska Native, Asian/Pacific Islander, and Hispanic women.
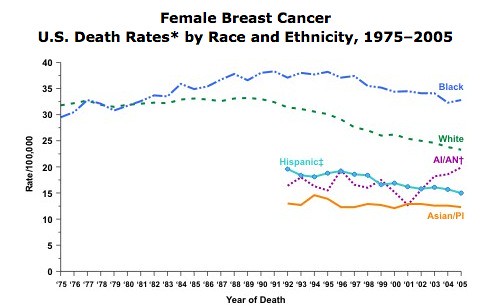
The graph below shows that in 2005, black women were more likely to die of breast cancer than any other group. White women had the second highest rate of deaths from breast cancer, followed by women who are American Indian/Alaska Native, Hispanic, and Asian/Pacific Islander.
A number of contributors to this disproportionate mortality have been proposed, including environmental toxin and pesticide exposure, more aggressive tumours, and later diagnosis. Most alarmingly, the mortality gap seems to be widening.
This week’s British Medical Journal (BMJ) has an important article today demonstrating one of the consequences of healthcare racism in the USA:
The researchers analysed national cancer records for 18,050 US women, aged 65 or older and otherwise non-disabled, who were diagnosed with early stage breast cancer during an eleven year period to 2002, and who received breast conserving surgery and radiotherapy, but not chemotherapy.
30% of the women in this study had to wait more than six weeks after their surgery before they could have radiotherapy. Delays greater than six weeks were associated with a modest but significant increase in local recurrence of the breast cancer.
The study also showed that there was a continuous relationship between radiotherapy delays and local recurrence; the sooner radiotherapy was started, the lower the risk of cancer recurrence, and this relationship was strong. This is concordant with previous studies.
So who was subject to these long, risky delays in treatment?
Sadly, the answer will not surprise you: Black women, Hispanic women, and poor women. Black women were almost 50% more likely to experience a longer than six week gap before radiotherapy treatment, and Hispanic women experienced a 30% increase in risk of delay.
The followup was only five years long in this study, and breast cancer tends to be a cancer that bides its time; the increase in risk (and in consequence mortality) may be greater, even much greater, with longer followup. In addition, as local recurrence risk tends to more common in younger women and this study focused on older women, the effect could be more pronounced in the total population of those with breast cancer. In addition, the study studied mostly White women, as Black women tend to get their cancers younger and have a decreased likelihood of receiving breast-conserving surgery and radiotherapy. In other words, this study was set up in a way that made it, in some ways, particularly difficult to find a significant difference in the effect they were looking at; the fact that they still found one means that the effect is likely to be really quite pronounced.
The accompanying BMJ editorial by Ruth H Jack and Lars Holmberg[2] goes on to suggest one possible model of healthcare delivery that might alleviate these delays:
One good example of how practices can be improved is the Rapid Response Radiotherapy programme in Ontario. This programme has drastically shortened waiting times for patients having palliative radiotherapy by restructuring the referral process so that many patients are treated on the same day as their consultation.9 Countries where disconnected systems are responsible for different aspects of treatment will find it more difficult to ensure that diagnosis, referral, and treatment are not subject to delay.
++++++++++++++++++++++++++++++++++++++++++
[1] Impact of interval from breast conserving surgery to radiotherapy on local recurrence in older women with breast cancer: retrospective cohort analysis
Rinaa S Punglia, Akiko M Saito, Bridget A Neville, Craig C Earle, Jane C Weeks.
BMJ 2010;340:c845; Published 2 March 2010,
doi:10.1136/bmj.c845
[2] Waiting times for radiotherapy after breast cancer
BMJ 2010;340:c1007
Published 2 March 2010,
doi:10.1136/bmj.c1007

![[aut_concept_chart.png]](http://2.bp.blogspot.com/_TnjsDMkGT2U/SMFkxbfhYCI/AAAAAAAAAO4/W_YrZEh1TNg/s1600/aut_concept_chart.png "AnneC's chart: Conceptualizing Autism") AnneC’s chart: Conceptualizing Autism, transcribed below[1. The chart reads in three columns, transcribed here:
AnneC’s chart: Conceptualizing Autism, transcribed below[1. The chart reads in three columns, transcribed here: